|
Links:
 Civil
War Medicine
Civil
War Medicine
 Death
to Dust: What Happens to Dead Bodies? Second Edition
Death
to Dust: What Happens to Dead Bodies? Second Edition
Treating
President Lincoln's Fatal Head Wound
By
Alfred Jay Bollet, M.D.
From: Civil War Medicine: Challenges and Triumphs
©Galen Press, Ltd., Tucson, AZ, 2002
 On
April 14, 1865, John Wilkes Booth shot President Abraham Lincoln
in the back of the head with a .41-caliber bullet fired from his
single-shot Derringer pistol. Lincoln and his wife were attending
a play at Ford's Theater in Washington, D.C., that night. Booth
chose a moment with loud laughter from the audience, which obscured
the sound of the pistol. The assassin immediately dropped the empty
Derringer and used a hunting knife to severely slash the upper arm
of Maj. Henry R. Rathbone (who was also in Lincoln's box). Booth
then jumped down to the stage. On
April 14, 1865, John Wilkes Booth shot President Abraham Lincoln
in the back of the head with a .41-caliber bullet fired from his
single-shot Derringer pistol. Lincoln and his wife were attending
a play at Ford's Theater in Washington, D.C., that night. Booth
chose a moment with loud laughter from the audience, which obscured
the sound of the pistol. The assassin immediately dropped the empty
Derringer and used a hunting knife to severely slash the upper arm
of Maj. Henry R. Rathbone (who was also in Lincoln's box). Booth
then jumped down to the stage.
Assistant Surgeon
Charles A. Leale, one of two army surgeons in the audience, was
the first to reach the president. Leale, who was in charge of the
officer's ward at Armory Square Hospital, had obtained special training
in head wound treatment at New York's Bellevue Hospital under Dr.
Frank Hastings Hamilton. Leale noted that Lincoln was not breathing
and, because he had seen Booth brandishing a bloody knife as well
as Major Rathbone's bleeding arm, he thought at first that Lincoln
must have been stabbed. He loosened Lincoln's collar and shirt but,
finding no stab wound and seeing blood on his shoulder and an enlarged
right pupil (an indicator of increased intracranial pressure, known
as a "blown pupil"), he then suspected a head wound. When
Leale palpated the back of Lincoln's head, he felt the ball's entry
wound. When he tried to probe the wound with his fingertip, feeling
for the bullet, he dislodged a blood clot and Lincoln began to breathe
again.
 Leale
did not find the ball under the scalp or when he probed the skull
wound as far as his fifth finger reached. He noted in his reports
to the surgeon general and to a Congressional investigating committee
that the skull wound had smooth edges. This indicates that his finger
did not penetrate deeply, since the fracture of the inner table
of the skull would have had sharp beveled edges and would have injured
his finger. (Indeed, the autopsy revealed such changes in the inside
layer of the bone of the skull.) Leale
did not find the ball under the scalp or when he probed the skull
wound as far as his fifth finger reached. He noted in his reports
to the surgeon general and to a Congressional investigating committee
that the skull wound had smooth edges. This indicates that his finger
did not penetrate deeply, since the fracture of the inner table
of the skull would have had sharp beveled edges and would have injured
his finger. (Indeed, the autopsy revealed such changes in the inside
layer of the bone of the skull.)
Dr. Charles S. Taft,
the second army surgeon to reach the President's box, also noted
that one pupil was large and the other very small, but he recorded
that the left was widely dilated and the right was contracted. Both
surgeons realized that the bullet had entered the brain from behind
and thought that it had probably blasted pieces of the skull into
the right orbit, since the right eye was protruding and discolored.
Both agreed that the wound would be fatal.
 Lincoln
was tenderly carried across the street to a rooming house and laid
diagonally across the small bed, semi-sitting with a wedge of pillows
under his head and shoulders. At about 1:00 a.m., three hours after
being shot, Lincoln experienced an episode of general twitching,
with arm spasms which tended to turn his palms down (pronate them).
Afterwards, his pupils became fixed, dilated, and non-reactive to
light. These findings can be interpreted as meaning that Lincoln
was now decerebrate and progressing rapidly toward death. Lincoln
was tenderly carried across the street to a rooming house and laid
diagonally across the small bed, semi-sitting with a wedge of pillows
under his head and shoulders. At about 1:00 a.m., three hours after
being shot, Lincoln experienced an episode of general twitching,
with arm spasms which tended to turn his palms down (pronate them).
Afterwards, his pupils became fixed, dilated, and non-reactive to
light. These findings can be interpreted as meaning that Lincoln
was now decerebrate and progressing rapidly toward death.
At about 2:00 a.m.,
Surgeon General Joseph Barnes used a silver probe to investigate
the wound and to keep a clot from forming; later he introduced a
porcelain-tipped Nélaton probe deep into the bullet track.
The probe hit something solid, but there was no mark of lead on
it and Barnes concluded that it had struck a piece of bone. No further
attempts were made to find the bullet. The wound continued to ooze
blood and brain tissue. Lincoln's breathing became intermittent
and finally ceased altogether at 7:22 a.m. on April 15.
Lincoln's body was
removed to the White House and placed on his bed in the "Lincoln
bedroom," where Dr. Joseph J. Woodward of the Surgeon General's
Office performed an autopsy beginning at noon; it was limited to
the head. (Two weeks after performing the autopsy on President Lincoln,
Dr. Woodward autopsied the body of John Wilkes Booth aboard The
Montauk, a Federal monitor.) Woodward thought that the ball, which
had fallen out when the skull was opened, had lodged above the left
eye, but Surgeon General Barnes recorded that he thought the ball
had probably lodged above the right eye.
President Lincoln's
family physician, Dr. Robert King Stone, was also present at the
autopsy. His handwritten notes and a diagram of some of his observations
were found and published almost exactly 100 years after the event.
His description is very similar to Woodward's: he states that the
bullet was lodged in brain substance on the left side. These contradictions
have never been resolved. As Dr. John K. Lattimer, the most detailed
and informed reviewer of these observations, pointed out, all those
involved in the care of President Lincoln and in the autopsy were
extremely upset, under severe emotional stress, and had marked sleep
deprivation by the time of the autopsy.
Woodward recorded
that the bullet had entered the back of the head (the occipital
bone) and passed through the entire length of the brain and through
the right lateral ventricle (a brain cavity normally filled with
spinal fluid); both ventricles and the track of the ball through
the brain tissue were filled with clotted blood and contained several
small bone fragments. There was a thick subdural clot on the surface
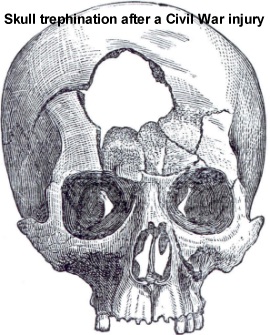
of the brain. The roofs of both eye sockets (the orbital plates)
were fractured and fragments of bone pushed up into the brain.
Debris found inside
the head included the flattened ball, a sharp-edged disk of metal
sheared from the ball, a burnt cloth patch that had been wrapped
around the ball in the Derringer, large sharp-edged disks of bone
from the inner table of the skull, and numerous small sharp fragments
of thin (cancellous) bone from the plates of the skull. These fragments
were photographed and preserved. According to experienced coroners,
orbital plate fractures are frequent after bullet wounds to the
head. They probably occur because of the pressure changes resulting
from distortion of the skull as a result of the impact of the bullet
and displacement of intracerebral tissues.
 The
treatment of President Lincoln's head wound was the typical approach
during the Civil War and for a long time afterward. Since the bullet
had penetrated the entire length of the brain from back to front
and there was extensive hemorrhage into the tissue and ventricles
within the brain, there was no hope of recovery. Such wounds were
virtually always fatal during the Civil War, and most still are
today. The attempts to find the bullet were routine at the time,
although the Surgical Section of Medical and Surgical History contains
descriptions of twenty cases in which the bullet was allowed to
remain in the cranium. However, in most of the cases, there was
considerable or total disability, usually accompanied by convulsions
or paralysis, and most patients died within a few years of the injury. The
treatment of President Lincoln's head wound was the typical approach
during the Civil War and for a long time afterward. Since the bullet
had penetrated the entire length of the brain from back to front
and there was extensive hemorrhage into the tissue and ventricles
within the brain, there was no hope of recovery. Such wounds were
virtually always fatal during the Civil War, and most still are
today. The attempts to find the bullet were routine at the time,
although the Surgical Section of Medical and Surgical History contains
descriptions of twenty cases in which the bullet was allowed to
remain in the cranium. However, in most of the cases, there was
considerable or total disability, usually accompanied by convulsions
or paralysis, and most patients died within a few years of the injury.
By the end
of the 1800s, with x-rays to help locate the missile, surgeons knew
that trying to remove a bullet deeply embedded in the brain caused
too much harm and they would leave it there, sometimes with good
results. While the attempts to find the bullet in President Lincoln's
head were harmful, no one really believes they affected the outcome.
|
